









Back In the Game Sooner: Nonsurgical Treatment for Sports Injuries and Arthritis
- Details
- Written by: Joanne Wallenstein
- Category: Health
 “As people stay active longer, we’re seeing more injuries from both sports and aging joints,” says Dr. Jonathan Holder (pictured), an orthopedic surgeon who frequently treats sports-related injuries, arthritis, and osteoporosis.
“As people stay active longer, we’re seeing more injuries from both sports and aging joints,” says Dr. Jonathan Holder (pictured), an orthopedic surgeon who frequently treats sports-related injuries, arthritis, and osteoporosis.
Sports Injuries at Every Age
From young athletes to weekend warriors, knee, ankle, and wrist injuries are common. These range from ligament and tendon damage to sprains and overuse injuries. Many patients benefit from nonsurgical approaches—such as injection-based therapies that support the body’s natural healing process—helping reduce pain and downtime and, in some cases, avoid surgery altogether.
“Advances in nonsurgical care are helping many patients recover faster and safely maintain their activity.”
Caring for Aging Joints and Bones
In older adults, fractures from minor falls and chronic pain from arthritis are common. Nonsurgical treatments, like hyaluronic acid injections, help improve joint function, reduce pain, and sometimes delay the need for surgery. “Treatment isn’t just about relieving pain,” Dr. Holder notes. “We also focus on prevention— improving bone strength, balance, and flexibility to reduce future injuries.”
A Faster, More Convenient Path to Recovery
Early diagnosis is key. Imaging—available onsite at multiple White Plains Hospital Physician Associates (WPHPA) locations—and physical therapy (offered by Burke Rehabilitation at WPHPA of West Harrison, WPHPA of Scarsdale and White Plains Hospital Medical & Wellness in Armonk) support faster, more coordinated care, often beginning the same day. “Reducing delays makes a huge difference,” Dr. Holder says. “Patients leave with a clear plan and confidence that they’re on the right path.” While many patients improve with nonsurgical care, Dr. Holder and his colleagues at WPHPA also provide advanced surgical treatment when needed, guiding patients seamlessly from diagnosis to recovery.
These two treatments boost healing without surgery:
Platelet-Rich Plasma (PRP) Therapy
PRP uses a patient’s own concentrated platelets to support healing in chronic tendon, ligament, muscle, and early joint injuries. It’s an in-office treatment with minimal downtime, and results typically develop gradually over several weeks.
Hyaluronic Acid (HA) Injections
Hyaluronic acid injections help lubricate arthritic joints— most often the knee—to reduce pain and improve movement. Relief may begin within weeks and can last several months, offering a non-surgical option for managing osteoarthritis.
To make an appointment with Dr. Holder, call 914-849-7897.
This story originally appeared in Health Matters, a White Plains Hospital publication.
Letter to the Editor: Splicing the Data on Reveal Math
- Details
- Written by: Joanne Wallenstein
- Category: Health
 (This letter was submitted by Daniel Rothman)
(This letter was submitted by Daniel Rothman)
To the Editor,
Scarsdale is known for academic excellence, and we need a board that will continue to elevate it. We need Board members who will work with parents, educators and administrators to improve pathways for parent input and district-wide communication. Most importantly, they must ask respectful questions and hold the administration accountable when results slip.
That is why I am voting for Kevin Ziegler and Omer Wiczyk.
The district celebrates that Scarsdale students are still "Proficient" under Reveal Math. Across Grades 3 through 6, the share of students scoring "Proficient" averaged 89.5% across the three years before Reveal (2017-18, 2018-19, 2021-22)*. Across the three years since Reveal was adopted (2022-23, 2023-24, 2024-25), that number climbed slightly to 91.9%. The district cites this as proof the curriculum is working.
But this celebration of "Proficient" is a celebration of mediocrity. On New York State's four-point scale, "Proficient" lumps Level 3 (meets standard, i.e. passing) with Level 4 (exceeds standard, i.e. excellent) into one number. Across the same three pre-Reveal years, Grades 3 through 6 averaged 59.3% excellent (Level 4). Across the three Reveal years, the average dropped to 50.1% excellent (Level 4). This is a 9.2 point reduction in excellence for our lower grades.
Parents have repeatedly asked the district to explain why they believe Reveal is the most effective math program for our children. It is safe to say the rollout has been bumpy at best. A year ago, at the district's June 2025 Reveal Math Coffee, parents put forward three concrete testing proposals. All three were declined, and no alternatives were shared. A school administration that refuses to critically evaluate its own curriculum and treats parent concerns as a nuisance is one that needs a change. Erica German has volunteered many hours, and I genuinely thank her for her service. But being a long-time insider is the opposite of what is needed. The insiders are the ones who told parents we weren’t qualified to engage. They are not going to be the ones who change that culture. We need a board willing to ask questions and constructively develop solutions.
After speaking with Kevin and Omer, I am confident that if elected they will critically assess the data, ask respectful questions, and preserve the values that define our schools: academic excellence, intellectual curiosity, and an environment where students are challenged. More importantly, Kevin & Omer are already building those communication pathways between parents, administrators and the Board. They came to my neighborhood to seek out a diversity of perspectives. That is why I will be voting for them, and if you want to continue having some of the best schools in the country (keeping your property values high), you will too.
Daniel Rothman
172 Boulevard
* Source: NYSED Data Site, data.nysed.gov, Scarsdale UFSD Grades 3 through 6 Math Assessment, six years of district report cards. Institution ID 800000034921. Pre-Reveal years: 2017-18, 2018-19, 2021-22. Reveal years: 2022-23, 2023-24, 2024-25. 2019-20 cancelled for COVID. 2020-21 excluded due to low participation. Same data the district uses.
Commenting on Rothman's letter, Mayra Kirkendall Rodriguez said the following:
Correlation Is Not Causation
I read Mr. Rothman’s letter with great interest. It seems to be a partial data analysis of some Scarsdale math test scores combined with a campaign letter and a critique of the Scarsdale School District Administration and current school board. Essentially, Mr. Rothman states that elementary school math scores in the Scarsdale School District have declined since the Reveal Math curriculum was rolled out in the District. Yet, correlation is not causation.
Without seeing grade-by-grade data, variance, subgroup performance, or statewide comparisons, it is difficult to see if the change in math test scores is due to the Reveal Math curriculum itself or whether there are other factors influencing the data.
Given the concern of some elementary school parents about the Reveal Math curriculum, conducting data analysis is a very worthy endeavor. Mr. Rothman’s disaggregation of Level 3 and Level 4 scores rather than treating “Proficient” as a monolith is a valid data analysis methodology. Using a combined metric can easily mask a shift from "excellent" to merely "passing." Asking for a granular breakdown when analyzing data sets is fair, relevant, and can be very useful.
For individuals wanting to analyze the Reveal Math curriculum dispassionately, however, there are several factors that would be worth addressing in a subsequent data analysis iteration to come up with an assessment of the Reveal Math curriculum.
I include my questions and observations here.
https://docs.google.com/document/d/1yjbOGe_EQWpSmyC26Qp3hWN4JqFedj5-6RWpo7Ltmaw/edit?usp=sharing That document also includes a list I researched and compiled of almost 300 cities and counties that have implemented the Reveal Math curriculum across the U.S.
And Tina Lin had this to say:
I have to take issue with Mr. Rothman's statement that "insiders told parents that they aren't qualified to engage". As an "insider", I don't think that anyone on the PTA would ever make such a statement. The PTA celebrates how involved, knowledgeable and qualified our community is, and we have always encouraged parental involvement and voice. It's the definition of the PTA. Further, being a long term volunteer does NOT preclude Erica German from asking questions and constructively developing solutions.
In fact, she is probably better positioned to ask the right questions and develop effective solutions faster because she already has a foundation. Erica's qualifications should also not be reduced to being a "PTA volunteer." She is a psychiatrist, who also understands child development and is a specialist in listening and communication. As a parent of a 4th grader and a member of the PTC EC, Erica is perfectly aware of and has communicated to the administration about parents' concerns with Reveal Math, but the reality is that PTC/PTAs don't have a "vote" on the Board. She has done what she can: initiated group forums, facilitated individual parent meetings, and has proactively provided feedback to Drew & Edgar. She's running for BOE to be able to make a larger impact.
Finally, I also have to strongly question Mr. Rothman's assertion that Kevin and Omer showing up for some meet and greets in the past month makes them better connected to the community than Erica German, who has been in the community, in the schools, showing up for BOE meetings, talking to parents, day in and day out for 17 years. Everyone should support who they want for the Board, and our community has some terrific options this year. However, please do not try to garner support for your candidates by playing on parents' frustration with Reveal Math and then making false statements about what Erica German represents and what she intends to and is able to do.
Recycling Tip: Paper Towels and Napkins Can Go in the Food Scrap Bin
- Details
- Written by: Conservation Advisory Council
- Category: Health
 Recycling Tip of the Week: Paper towels, paper napkins and tissues do NOT go in paper recycling—They can go in the food scraps bin
Recycling Tip of the Week: Paper towels, paper napkins and tissues do NOT go in paper recycling—They can go in the food scraps bin
Paper towels, paper napkins and tissues should not be placed in paper recycling. Whether they are unused or used, they cannot be recycled. These are "end of life" paper products as they are made from highly processed wood pulp that creates extremely short, weak fiber which cannot be turned into new paper products. They can, however, be placed in food scrap recycling as long as they have not been contaminated with cleaning products or other chemicals. Since the fibers come from wood, they can be composted. Placing uncontaminated paper towels, paper napkins and tissues into food scrap recycling will guarantee that these products will be reused as compost. If you have any questions, please email composting@scarsdale.gov.
Do You Really Need Vitamins and Supplements? A Physician’s Take
- Details
- Written by: Joanne Wallenstein
- Category: Health
 As a physician, one of the most common questions I hear is: “Should I be taking a daily multivitamin?” With nearly 75% of Americans using dietary supplements, it’s clear this is top of mind for many people.
As a physician, one of the most common questions I hear is: “Should I be taking a daily multivitamin?” With nearly 75% of Americans using dietary supplements, it’s clear this is top of mind for many people.
The Truth About Multivitamins
Despite their popularity, research shows that multivitamins do not significantly reduce the risk of major diseases like cancer or heart disease. In other words, for most healthy adults, taking a daily multivitamin isn’t the shortcut to better health that many hope it is. However, while most young adults do not require multivitamins, new research does demonstrate the benefits of multivitamins for health and longevity in adults over 50.
Why “More” Isn’t Always Better
Many people assume over-the-counter supplements are completely harmless, but that is not always true. Supplements can interact with medications, cause side effects, or even lead to excessive intake of certain nutrients.
Where Your Nutrients Should Come From
In my clinical experience, the best way to get essential vitamins and minerals is through a well-balanced diet. Focus on:
• Fruits and vegetables
• Whole grains
• Nuts and seeds
• Lean proteins
• Dairy or dairy alternatives
These foods provide a combination of nutrients, fiber, and antioxidants that supplements simply can’t replicate. Pair this with regular exercise and maintaining a healthy weight, and you have the true foundation of long-term health.
When Supplements Do Make Sense
There are situations when supplement can be beneficial:
• Cold and flu season: Vitamin C and zinc may help reduce symptom duration
• Pregnancy: Folic acid is essential for fetal development
• Dietary restrictions: Vegans and vegetarians may need B12, iron, or other nutrients that may be lacking or harder to absorb from plant-based foods
• Medical conditions: People with malabsorption issues or those who’ve had bariatric surgery may require targeted supplementation
The Bottom Line
If you’re generally healthy, you likely don’t need a daily multivitamin. Instead, focus on what truly matters:
• Eating a nutrient-rich diet
• Staying physically active
• Maintaining a healthy weight
Think of supplements as a targeted tool, not a daily necessity. When used correctly, they can support your health, but they should never replace the basics.
That’s why I always recommend talking with your doctor before starting any new supplement. A simple blood test can often determine whether you actually need one—and which type is best.
Dr. Thomas Karoff is an internal medicine physician at Scarsdale Medical Group/White Plains Hospital Physician Associates. To make an appointment, call 914.723.8100.
This article originally appeared on Health Matters, a White Plains Hospital publication.
Students Showcase Research Project at Annual Syposium
- Details
- Written by: Harrison Greebel
- Category: Health
 Sonja XieOn Monday, April 13th Scarsdale High School Juniors who are enrolled in the three-year Science Research program hosted the Annual Science Research Symposium. During this event, Seniors showcased their independent, mentor-guided research projects, including slide presentations, scientific papers and award-winning work. The event serves as a platform for students to share their scientific contributions with the community, parents and Scarsdale High School faculty.
Sonja XieOn Monday, April 13th Scarsdale High School Juniors who are enrolled in the three-year Science Research program hosted the Annual Science Research Symposium. During this event, Seniors showcased their independent, mentor-guided research projects, including slide presentations, scientific papers and award-winning work. The event serves as a platform for students to share their scientific contributions with the community, parents and Scarsdale High School faculty.
The symposium is the culmination of a three-year elective course, which starts in the sophomore year, focusing on in-depth, student-led research in science, technology, engineering, mathematics, psychology or certain social-sciences. The event highlights the depths of research achieved by students enrolled in the program, choosing topics to study, learning to read scientific literature, identifying mentors actively working in their chosen fields, conducting independent and original research and competing in competitions.
This year two SHS seniors received awards at the Regeneron Westchester Science and Engineering Fair. Rachel Rakower received a second place award and Sonja Xie received a third place award.
The program is designed for students with a high level of ambition and independence and offers them an opportunity to engage in college-level research. SHS juniors are responsible for organizing the symposium and focus on three core areas.The publicity committee is responsible for promoting the event; the program committee reviews abstracts and develops the printed program; and the technology committee creates the slideshows and prepares the website for presentations. The website will launch on June 1st and will showcase the seniors’ completed research as well as the projects that sophomores and juniors enrolled in the class will research during the upcoming summer.
I am researching the impact that online payment forms have on college students' spending habits. Specifically, I am analyzing whether platforms such as Venmo, Zelle and Paypal are causing college students to make irresponsible payments. I am trying to determine whether these platforms are causing an increase in impulse purchases or whether these platforms are preventing college students from developing key financial skills that will impact them later in their lives.
Below are summaries of some of the senior presentations. If you are interested, you are encouraged to connect with the presenters or learn more when the website launches.
 Sophie Lammer
Sophie Lammer
Sonja Xie
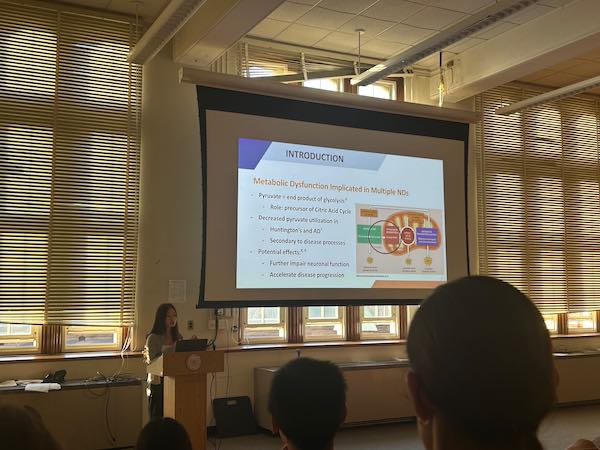
Topic: Neurite Degeneration Following UK-5099 Inhibition of the Mitochondrial Pyruvate Carrier Reveals Metabolic Thresholds for Neuronal Integrity
Summary: Neurodegenerative disorders are characterized by the progressive loss of neurites—the essential communication projections of nerve cells—which is linked to impaired energy metabolism. To investigate this, primary cortical neurons were treated with UK-5099, a synthetic inhibitor of the mitochondrial pyruvate carrier (MPC), revealing significant, dose-dependent structural loss. These results suggest that mitochondrial pyruvate transport is a key regulator of neuronal integrity and a potential target for neuroprotective therapies.
 Julia Wu-Oswald
Julia Wu-Oswald
Julia Wu-Oswald
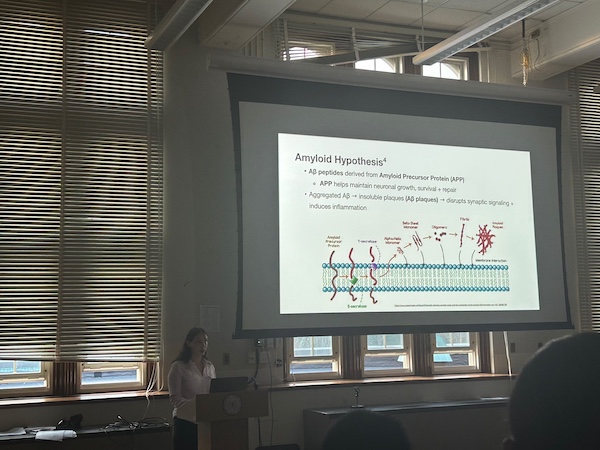
Topic: Lipids in Alzheimer's Disease
Summary: In Alzheimer's Disease, an abnormal accumulation of lipids strongly correlates with cognitive decline and the toxic build-up of amyloid-beta plaques. Previous in vitro studies showed that applying avasimibe inhibits the creation of cholesteryl esters within glial cell lipid droplets, which helps microglia (immune cells) more effectively clear away amyloid-beta. However, my in vitro study found that newly synthesized avasimibe derivatives were ineffective in increasing this uptake, failing to assist microglia in clearing the plaques and leaving the brain vulnerable to continued toxicity.
Sophie Lammer
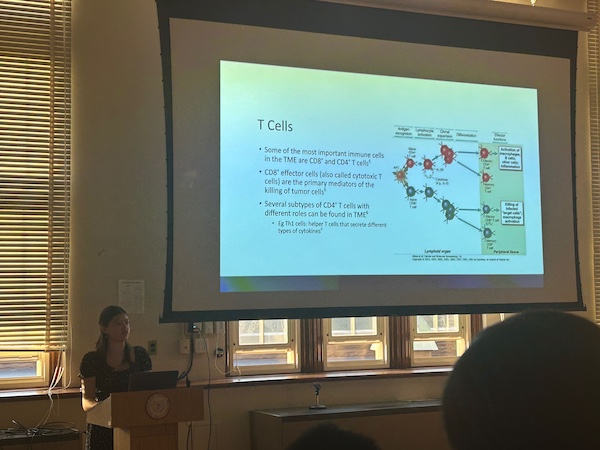
Topic: Phenotyping of Cocultured Chronically Activated CD8+ and CD4+ T Cells In Vitro
Summary: CD8+ and CD4+ T cells are the immune system's most important defenders against cancer, but over time, their tumor-killing abilities become exhausted from prolonged activation. My in vitro experiment directly explored how this T-cell exhaustion is driven by harmful changes in the cells' lipid metabolism. By characterizing these metabolic and structural changes, my research elucidates exactly how these T cells fail to properly regulate the anti-tumor immune
response.
Peter Lin
Topic: Microbiology
Summary: The pathogen Fusobacterium nucleatum has been strongly linked with colon tumors, but the molecular mechanisms promoting this tumorigenesis remain unclear. This study investigates how F. nucleatum may promote tumor development by disrupting RNA interference (RNAi), an important regulatory pathway in gene expression. Results show that exposure to the pathogen prevents the formation of key RNAi complexes, suggesting a novel mechanism mediating host-pathogen interactions in cancer development.
Overall it was an amazing night to showcase our wonderful outgoing seniors' work.
Contirubted by By: Harrison E. Greebel SHS Class of 2027
