









The Battle Against Coronary Artery Disease
- Details
- Written by: Joanne Wallenstein
- Category: Health
 Coronary artery disease (CAD), also known as atherosclerosis, is the most common type of heart disease, with the CDC reporting that it killed 375,476 people in 2021. About 5% of those aged 20 and older have CAD – but many may not even be aware of it until serious symptoms occur.
Coronary artery disease (CAD), also known as atherosclerosis, is the most common type of heart disease, with the CDC reporting that it killed 375,476 people in 2021. About 5% of those aged 20 and older have CAD – but many may not even be aware of it until serious symptoms occur.
In fact, CAD may take place over decades, as it involves the buildup of plaque. Plaque is made of several substances, including cholesterol. Plaque buildup can start at an early age and is caused by a combination of genetic and lifestyle risk factors. As plaque builds up over time, the arteries become increasingly narrow; the resulting poor blood flow to the heart can result in angina (chest pain) as well as blood clots, further blocking the arteries and possibly leading to a heart attack.
Indeed, many symptoms of CAD, are similar to those of a heart attack: in addition to chest pain, they may experience tightness in the chest during exertion, shortness of breath, fatigue, and lightheadedness. People who experience these symptoms during exertion may feel relief when they stop physical activity, but if it recurs when they begin exerting themselves, it may be time to visit their primary care physician or a cardiologist.
Causes of CAD include several modifiable factors: high blood pressure, diabetes, smoking, and a lack of exercise can all contribute to developing the disease. In addition, a family history of CAD (primiarly in your parents or siblings) can also be a significant consideration.
Furthermore, men are at a higher risk for developing CAD, although menopause increases a woman’s risk of developing the disease due to the many hormonal changes they experience during and after menopause.
Determining a given patient’s risk for developing (or already having) CAD can involve a number of tests, including a routine blood test, which will reveal if they have low-density lipoprotein (LDL) – commonly called the “bad” cholesterol” –, high-density lipoprotein (HCL) chloesterol (the “good” cholesterol). We also are now checking other markers in the blood like lipoprotein (a) and C-Reactive Protein (CRP), which is an indication of unusual inflammation.
Another test I perform is a coronary calcium score, which is a CT scan that looks at calcification in order to assess your risk of a heart attack over 10 years. There are three levels of results: mild is any number between one and 100; moderate is anywhere from 100 to 300; and severe is any number greater than 300; in fact, a severe score can be several hundred, indicating that action should be taken quickly.
Prevention and Treatment
A good diet can help reduce your risk of coronary artery disease. I recommend eating vegetables, fruits, fish, and legumes. It is also important to get enough exercise; I recommend at least 150 minutes of moderate aerobic activity, or 75 minutes of vigorous aerobic activity, a week. As is always the case, the long-term use of cigarettes or other nicotine products can have serious health risks, including the development or acceleration of CAD.
If a person’s case of CAD is found to be especially concerning, there are several prudent treatment options. These can range from taking medications to undergoing surgery. If you are concerned that you may be at risk for, or already have, CAD, ask your doctor to perform an EKG, bloodwork, and/or a calcium score test.
Dr. Gregory Pontone is a noninvasive cardiologist and the Associate Medical Director of Ambulatory Quality and Physician Services at White Plains Hospital. To make an appointment, call 914-849-4800.
Health Matters
The original version of this article was published in Health Matters, a White Plains Hospital publication.
Pickleball Pilot Program To Launch at Crossway Tennis Courts
- Details
- Written by: Joanne Wallenstein
- Category: Health
 Good news for Pickleball fans. The hard tennis courts at Crossway will be converted to pickleball courts for a pilot program starting on September 18 Through October 31. In order to participate Scarsdale residents must purchase a crossway pickleball pilot permit for a fee of $30. Residents wishing to take advantage of this program opportunity can purchase a permit online here: https://www.scarsdale.com/208/Tennis-Platform-Tennis-Pickleball or at the Department of Parks Recreation and Conservation. Located at 244 Heathcoat Road.
Good news for Pickleball fans. The hard tennis courts at Crossway will be converted to pickleball courts for a pilot program starting on September 18 Through October 31. In order to participate Scarsdale residents must purchase a crossway pickleball pilot permit for a fee of $30. Residents wishing to take advantage of this program opportunity can purchase a permit online here: https://www.scarsdale.com/208/Tennis-Platform-Tennis-Pickleball or at the Department of Parks Recreation and Conservation. Located at 244 Heathcoat Road.
Only Crossway pickleball permit holders will be able to reserve court time and reservations can be made here: https://secure.rec1.com/NY/village-of-scarsdale-ny/catalog
The hours of play for the pickleball pilot program are 9am to dusk daily. Players without permits must show proof of Scarsdale residency, and the fee is $15 per player per hour. Non resident guests may only play on weekends between noon and 4pm and must play with a resident. The non-resident guests fee is $20 per player per hour. All players must check in with the attendant before playing.
Enjoy pickleball this fall and sign up today. Please call the Parks Recreation and Conservation Department with any questions you can reach our staff at 914-722-1160.
Dealing with a Child’s Food Allergies
- Details
- Written by: Joanne Wallenstein
- Category: Health
 (Submitted by Debra Etelson, Pediatrics at White Plains Hospital.)
(Submitted by Debra Etelson, Pediatrics at White Plains Hospital.)
Many parents and guardians, especially those with children going to daycare or school for the first time, are understandably concerned about whether the facility, its staff, and its other attendees are taking proper precautions when it comes to food allergens.
The good news is that any reputable, licensed establishment – by law – must do so. But that does not necessarily mean that one’s anxiety can simply be put away.
According to the nonprofit Food Allergy Research and Education (FARE), about 8% of children under the age of 18 have food allergies – equal to one in 13 children, or approximately two in every classroom. Eggs, milk, and peanuts are among the most common causes of food allergies in children, with wheat, soy, and tree nuts also included. Fish and shellfish are also on the list, though of course those are rarely served in schools or daycare centers.
Determining what foods your child may be allergic to can be complicated, but it needn’t be. Obviously if the child suddenly has trouble breathing, or experiences cramps, swelling, vomiting or diarrhea, a trip to the emergency room is necessary. But before such symptoms occur, a simple blood test or a scratch test performed by an allergist can raise the appropriate red flags.
Research has shown that children may outgrow some of these allergies before they’re five, although allergies to peanuts, tree nuts, fish and shellfish are usually lifelong.
Follow-up tests for someone who does have a food allergy usually take place every one to two years, and pediatricians will review allergies at each visit to track any changes. If the child has outgrown an allergy, there may be whole new edible worlds for them to explore – liberalizing a kid’s diet can be amazing.
Some food sensitivities and/or allergies may not be immediately apparent. Hives or tongue-swelling may occur when eating certain fruits and vegetables, but those reactions rarely progress to something more serious. You may see a reaction to raw carrots or apples, but not cooked ones, as cooking reduces the allergenic proteins and thus lowers the impact they have on the immune system.
When Kids Are in Someone Else’s Care
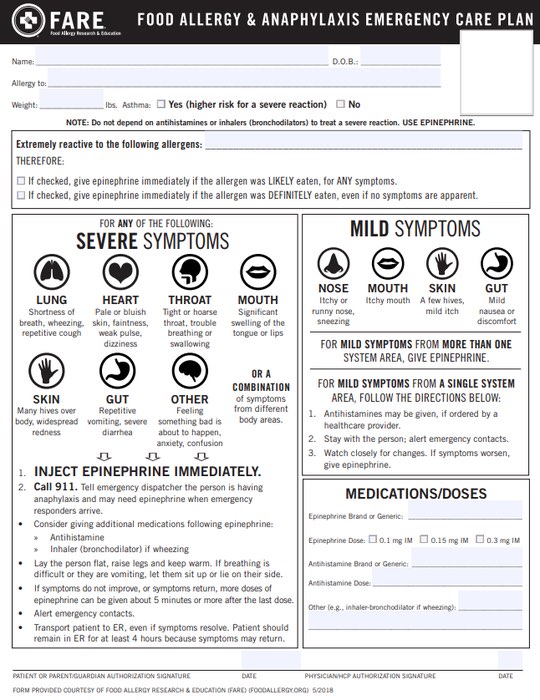
It may be relatively easy to monitor your child’s food intake at home, but what if they’re off to school or a playdate? Schools require the completion of a food allergy sheet like the one below before the term begins. This, along with a supply of Benadryl and/or an EpiPen, should help ease fears about your child being away for the day. In addition, many schools now prohibit peanuts and some other allergy-producing foods from the premises, eliminating the chances of an airborne infection.
Similarly, if your child is going to another home where you will not be present, converse with that caregiver and provide the appropriate medications. In all cases, remember that EpiPens are effective for 12 to 18 months, and like any other medication, will likely require a refill/replacement somewhere down the line. Also keep in mind that as your child ages, they begin to seek more independence, generally when they’re 10 or 11. That means they may don’t always carry their EpiPen or medication with them, so take the time to explain the importance of responsibility (and not just in this area of life!).
The FDA’s Pulmonary-Allergy Drug Advisory Committee (PADAC) voted 16-6 in favor for adults, and 17-5 in favor for children (under 18 years of age and weighing 66 or more pounds), acknowledging that available data supported a favorable benefit-risk assessment for neffy in the treatment of severe allergic reaction (Type 1), including anaphylaxis, for adults and children who weigh more than 66 pounds.
 Taking care of a child with a food allergy can be challenging, but being aware of what’s available and discussing the issues frankly with a pediatrician and other caregivers in your kid’s life should take at least a little worry out of the equation.
Taking care of a child with a food allergy can be challenging, but being aware of what’s available and discussing the issues frankly with a pediatrician and other caregivers in your kid’s life should take at least a little worry out of the equation.
Dr. Debra Etelson is a board-certified pediatrician at White Plains Physician Services in Somers. To make an appointment, call 914-849-7075.
Health Matters
The original version of this article was published in Health Matters, a White Plains Hospital publication.
County Officials Confirm Bear Attack in Bedford
- Details
- Written by: Joanne Wallenstein
- Category: Health
 This photo of a bear in Heathcote was taken in May, 2020The Westchester County Department of Health has confirmed today that the bear that attacked a 7-year old boy in Bedford as he played in his backyard on Tuesday August 22, 2023 has tested negative for rabies. The child is being treated and the bear was shot by authorities shortly after the attack.
This photo of a bear in Heathcote was taken in May, 2020The Westchester County Department of Health has confirmed today that the bear that attacked a 7-year old boy in Bedford as he played in his backyard on Tuesday August 22, 2023 has tested negative for rabies. The child is being treated and the bear was shot by authorities shortly after the attack.
Residents should never approach or have contact with a stray or wild animal. Residents who see a stray or wild animal acting strangely should alert local authorities to avoid possible exposure to rabies. Residents can also help by keeping their trashcan lids securely sealed, removing wild bird feeders, and avoid leaving pet food outdoors.
Health Commissioner Sherlita Amler, MD, said: “If you see an animal that is acting aggressively, stay away from it and contact local police immediately.”
Unusual behavior may be the first sign of rabies in an animal. A rabid animal may become either abnormally aggressive or unusually tame. It may lose fear of people and become excited and irritable, or, conversely appear particularly passive and lethargic. Staggering and frothing at the mouth are sometimes noted.
Any physical contact with a wild or unfamiliar animal should be reported to a health care provider. All animal bites or contacts with animals suspected of having rabies must be reported to the Westchester County Department of Health at (914) 813-5000, 24 hours a day.
Keeping pet rabies vaccinations up to date is also important for protection against rabies. New York State law requires dogs, cats and ferrets to be vaccinated against rabies and receive regular booster shots. For more information, go to www.westchestergov.com/health or call the RABIES INFOLINE at (914) 813-5010.
Freeing Patients from Shoulder Pain
- Details
- Written by: Joanne Wallenstein
- Category: Health
 The following was submitted by Dr. Michael Gott from White Plains Hospital
The following was submitted by Dr. Michael Gott from White Plains Hospital
Often when a patient hears the words “shoulder replacement,” they fear it means a loss of shoulder mobility for months and a long rehabilitation. Not so, assures Dr. Michael Gott, an Orthopedic Surgeon in the Center for Orthopedics and Spine Surgery at White Plains Hospital.
“Because it is not as common as knee or hip replacements, the misconception arises that this surgery entails removing and reattaching bones, tendons, and muscles,” he says. In fact, the procedure is technically a shoulder resurfacing, replacing just millimeters of damaged arthritic bone. During the procedure, Dr. Gott, guided by a CT scan, makes a tiny incision in the upper arm to insert a smooth titanium-alloy implant.
“CT-guided shoulder resurfacing is life-changing for those with end-stage shoulder arthritis, where the cartilage has worn away to create painful bone-on-bone friction,” says Dr. Gott.
Many of the patients the surgeon treats have had prior surgeries, multiple shoulder dislocations or just significant arthritis. Heavy lifting on the job or at the gym can exacerbate the pain. Some patients can no longer even lift their arms all the way up. These patients have exhausted all other options before electing to have the surgery.
“Injections only work for a few weeks or months, and medications have their own side effects,” Dr. Gott says. “And while physical therapy can be helpful for certain shoulder issues, it doesn’t address the damage to the joint that characterizes arthritis.”
For patients hesitant to embrace the idea of resurfacing, Dr. Gott points out the following advantages:
OUTPATIENT PROCEDURE. The patient receives local nerve blocks to numb the affected shoulder, undergoes an hour-long procedure, then receives a sling and returns home the same day. “Shoulder resurfacing requires fewer pain medications and a shorter recovery than even arthroscopic rotator-cuff repairs,” he explains.
MINIMALLY INVASIVE. Technological breakthroughs allow for tiny incisions and implants, removing a slice of bone that can fit on a fingernail. Rather than force metal into the bone, Dr. Gott slides titanium implants close to the joint.
PRECISION APPROACH. Dr. Gott’s team often creates 3D-printed models of a patient’s shoulder in advance to guide their approach during the procedure. “Studying the model cuts down on operating time and enhances accuracy. This focus on precision makes our outcomes even better,” he says.
RAPID RECOVERY. “As soon as they start physical therapy, patients tell me that they see a noticeable improvement in their strength and ranges of motion. They are also sleeping better within weeks, as opposed to months,” he notes. Following the procedure, patients typically require three months of supervised physical therapy, followed by exercises performed on their own as needed. They can then return to non-weight-bearing physical activities, such as golf, tennis, pickleball and racquet sports.
LOGISTICAL EASE. “Patients receive their consultations, CT scans, surgery, and follow-up care in the same location at our state-of-the-art Center for Advanced Medicine and Surgery,” Dr. Gott says. In addition to convenience, getting to know the care team promotes peace of mind for patients.
 In the end, Dr. Gott’s patients say they are grateful to have shrugged off their anxiety. “The most common feedback I hear from patients is that they only wish they had done the procedure sooner,” he says. “They not only recover — they bounce back even better.”
In the end, Dr. Gott’s patients say they are grateful to have shrugged off their anxiety. “The most common feedback I hear from patients is that they only wish they had done the procedure sooner,” he says. “They not only recover — they bounce back even better.”
Dr. Michael Gott Dr. Michael Gott is an orthopedic surgeon at the Center for Advanced Medicine and Surgery in White Plains. To make an appointment, call 914-849-7897.
Health Matters: The original version of this article was published in Health Matters, a White Plains Hospital publication.
